


Our Church's Vaccine Clinics
The Merits of focusing on Concrete efforts toward Justice

As some of you know, while this blog is focused primarily on my thoughts on more big-picture current events, I have another mailing list that focuses on personal and work-related things that I do. Many of you get those emails, but not all of you do (you can sign up here if interested). I realized some of you might find it interesting to read something that I wrote regarding my experience doing a series of vaccine clinics at my church earlier this year. If the tone is different, keep in mind the audience is slightly different from this blog
Vaccine Clinics
As you all may know from reading my past updates, the winter surge of COVID was particularly rough here in Los Angeles. COVID spread was not new here in Los Angeles: we had seen a minor surge at the beginning of COVID-19’s spread in the US in March of 2020 and another little surge in June/July of 2020. But the wave this past winter was significant: daily new cases in LA county were in the tens of thousands, hospitals and emergency rooms exceeded capacity, nursing homes were forced to receive COVID positive patients. It was grim wherever you looked.
Our neighborhood got hit especially hard. The high number of essential workers in restaurants and grocery stores combined with overcrowded housing (resulting from a pre-existing housing shortage) created a perfect storm for COVID spread. As a result, multiple families from my church saw several family members hospitalized, and a few had to undergo significant treatment to recover. And while our church thankfully did not lose any members to COVID, many had friends and extended family members who tragically lost their lives to COVID.
Thankfully, as December turned to January, we saw cases slow down somewhat as natural immunity levels rose, and many people adjusted their behavior to slow the spread. But the real promise that January brought to our community was the potential for widespread vaccination: vaccines enabled vulnerable people to be protected.
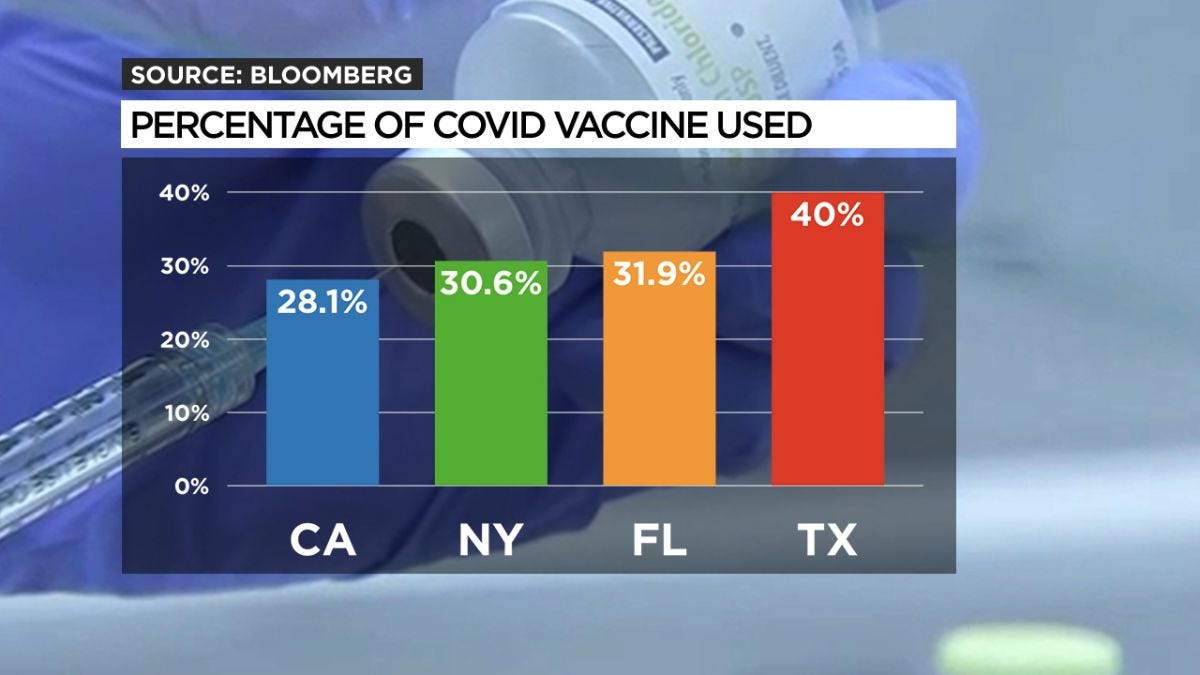
Unfortunately, it quickly became apparent that there were significant issues in California’s vaccine rollout. The rollout was very frustrating to watch. I believe that those who were running California’s vaccination program had all of the best intentions. But we should judge public policy on outcomes, not intentions. California wanted its vaccination rollout to prioritize equity: ensuring that marginalized groups got vaccinated at the same rate as more privileged groups. But despite those intentions, many of my neighbors were still unable to get vaccinated. Throughout the whole spring, the Eastside saw lower rates of vaccination than other parts of the city. Worse yet, it became apparent that California was not only failing to get vulnerable residents vaccinated but struggling to get ANY residents vaccinated. By mid-January, California had only distributed 25% of the doses that it had received from the federal government, and that rate only slowly rose over the spring.
The shortcoming of the rollout became the subject of heated debate here in California, and to this day, many disagree on the root causes of failure. I came to believe the state’s plan had three leading causes of failure:
1) First, the state created a complex framework for rationing doses of the vaccine under the assumption that if you allocated the doses to a specific group, they would naturally take advantage of that opportunity. But they underestimated the logistic difficulty that communities like mine would have in accessing the vaccine. Many did not have reliable internet to access appointment websites or have time during their workday for an appointment. Others did not have safe transportation (like a car) they could take to their appointment. Furthermore, many vulnerable residents are not primary English speakers; but the state did not translate necessary websites or sign-up forms into their language. Without addressing these issues, the rollout was always going to run into trouble
2) The attempts to micro-target who would get first access to the vaccine made it difficult for laypeople to figure out when they were eligible. California’s criteria involved factors like occupation, pre-existing conditions, and age. These categories frequently changed through the process. An average person with a busy, hectic life and responsibilities could not simply understand their place in line when the state was using such various categories. I had countless conversations with neighbors confused about whether their particular work function entitled them to a vaccine.
3) There was no widespread understanding of how to deal with (or even honestly talk about) vaccine hesitancy. From the beginning, it was evident that many folks on the Eastside were eager to get the vaccine as soon as they could. However, it was also clear that many others were hesitant to get the vaccine. There were many reasons for this: many people were skeptical of the attempts of the public health experts to explain the vaccine, they saw news reports that played up the side effects, and they had a history of negative interactions with doctors and the healthcare system. Sadly, initially, there was so much focus on rationing doses that there was little planning to address the long-term challenge of hesitancy.
One example is an older gentleman in our church I will call Jaime. Jaime approached our church about getting a vaccine because he struggled to figure out how to access one. Jaime was in his early 60s and was laid off from his food service last March due to COVID. He also had a pre-existing health condition that made him vulnerable to COVID. Neither of these made him eligible in the initial wave of vaccine eligibility. But even when he became eligible, he struggled to figure out how to get the vaccine. Jaime was a primary Spanish speaker, and he had no internet connection at home, which made it impossible to get information on where he could get a vaccine. His primary strategy for finding a vaccine was to call various helplines and clinics to see if they had appointments. When he finally did reach someone who helped him find a vaccine, the clinic’s location was in the San Fernando Valley, on the far side of Los Angeles. Jaime did not have a car, so getting to the appointment would have required him to take a two-hour bus ride in each direction, which was dangerous as a vulnerable person in the middle of a pandemic. He decided in the end to forgo the appointment.
For me, my instinct was initially to sit behind my keyboard and pontificate about all the shortcomings of California’s approach (all of which you can read on my blog). In many ways, it exemplified my frustrations with the discourse in America over the last 12 months. There is quite a bit of ink spilling in talking about racial and socioeconomic disparities and injustice in America, which is crucial to explore and understand! But there has been far less exploration of the complex reality of what it will take to address these disparities practically. It's easy to say you are committed to equity; it's a lot harder to find practical solutions to inequality that work in the crucible of the real world. Moreover, as California found out, policies pursued in the name of equity can often have unintended negative impacts. In this case, they sought equity without accounting for its effects on the speed of the vaccine rollout.


Turning Talk into Action
But I quickly became convinced that talk was cheap. Our church’s calling in our community was to solve this problem, to get involved in the messy work of trying to make things better in concrete and practical ways. So a team of folks started to explore seriously: could we invest our own time and resources as a church community trying to bring the vaccine into our community? We could increase the capacity of our community to access the vaccine. As long as the county gave us doses, we could ensure that shots went to vulnerable people and protected them from this terrible pandemic.
We spent the next few months creating a team: we had an emergency room doctor connected to our parent church to coordinate with the public health department, a pharmacist from San Diego to handle the doses, a medical mission group here in LA with a network of medical personnel who could administer vaccines, and the staff of our church and our sister church doing all we could to clear the path to make this a reality. We had to convince the public health department to trust us; we had to ensure that neighborhood groups trusted us enough to bring their people to get vaccinated! And we needed an army of volunteers who could help us since we had no grants from the local government, and we needed to ensure that all the necessary logistical work got done.
It is hard to understate how large this undertaking felt. I have precisely zero medical experience (not counting the armchair public health expertise many of us developed during the pandemic). I am more an “ideas” person than I am a “logistics” person, and vaccine clinics are very much a logistical enterprise. But I was blessed to see how a vast network of our people in LA united by a shared vision to come together to make everything happen.
Our three goals in hosting these clinics corresponded to the three problems we saw with California’s rollout:
Logistics: We wanted to make it as easy as possible for everyone in our community to sign up to get a vaccine at our clinic. The way I thought about it was “shifting the IT burden” from the community to our clinic. Instead of requiring patients to register and fill out pages of the paperwork beforehand, we worked to pare down our pre-clinic sign-up forms to just the information we needed to verify eligibility. We created our own IT system for intake forms and to track appointments. We then used our army of volunteers to register our patients, including patients who walked up the day of the clinic. Our volunteers included people who could translate the languages spoken by the many first-generation immigrants living in Lincolnprecisely Heights: Spanish, Vietnamese, Tagalog, Mandarin, Cantonese, and Taishanese. We had so many people who wanted to volunteer that we had to keep running counts of how many people we had in our church parking lot to make sure we could stay reasonably socially distanced!
Complexity: We knew that many people in our neighborhood did not fully understand the guidelines for eligibility for a vaccine and who were not. So we intentionally coordinated with as many local churches and community groups as possible to make sure that we leveraged existing networks of trust to get the word out. We also put our flyers on the street, ensuring that everyone eligible and interested heard that they could come. Ultimately, after multiple clinics, we built the trust with the public health that we were working hard to get doses to those in need. The department thus started to give us more leeway to use our best judgment when we confronted eligibility edge cases where people were clearly in need but didn’t have the documentation they needed to “prove” they were eligible. We saw this shift enable whole extended families to get vaccinated together.
Hesitancy: We believed that the most prominent tool we had to build trust in the vaccine was to leverage relationships. We thought that people would be much more likely to trust the vaccine when seeing their friends, family, pastors getting vaccinated in their community! We found that as people began to see those they knew and trusted getting vaccinated and sharing honestly about their experience, those who were skeptical or hesitant started to come around. We also found that by using our desire to be hospitable as a church, we could put people at ease. Our leaders, gifted in pastoring people, would welcome people as they came into line and talked about their own experience getting the shot and how they were doing OK. They would then circle and offer to speak and pray with them as they felt relief after getting the shot and often get to sit and pray with folks as they shared all they had gone through in the last year of craziness in their life and community.
One church member came to our first clinic unsure about getting vaccinated but ended up agreeing when we found we had gotten more extra doses we got from the vials than anticipated. This church member felt so relieved that they persistently spent the next four weeks trying to convince their skeptical spouse to get vaccinated until the day of our last clinic when the spouse finally gave in and came to get their dose!





Brittney’s Addendum
I (Thomas’ wife Brittney) asked if I could guest blog on his update letter, and he graciously agreed to let me ramble about my experience at one of the clinics our church held. And what an experience it was! Before we even started the day, I remember our Pastor saying to the volunteers that people were coming to our clinic because of that human touch we offered. People weren’t just a number here, and our clinic wasn’t just about getting people in and out as quickly and efficiently as possible. Instead, our goal was to show our community the love of Christ and welcome them into an environment that could feel scary and uncomfortable. I am by nature a get-it-done, efficiency-is-key type of woman and can quickly become brusque and no-nonsense when an important task is before me, but that framing helped set the tone for my role.
One story in particular sticks out to me and loosely ties into Thomas’s three goals on logistics, complexity, and hesitancy. As community members would wander down the street outside our church, we made a point to reach out to them to see if they wanted to receive a vaccine. Many agreed and ended up getting vaccinated. One such man was biking down the street when I flagged him and asked him if he wanted to receive a vaccine. I ended up taking to this man an hour and a half until he finally agreed to accept a shot. And I think it’s because of the love and care each person showed him at various touchpoints. He spent a copious amount of time talking (in Spanish) to our doctor about the risks. We had our nurse show him the exact dosage he would be receiving (only 0.5 mL, which is crazy to me still!). Our greeters at the front, myself included, asked him about some of his concerns and his hesitations and gave him some water to ease his anxiety. And finally, I went with him to answer all of the medical questions so he wouldn’t feel as alone in the process. I don’t think this man would have received the vaccine at one of Los Angeles’ mega-pod vaccination sites because it would’ve taken too much time and energy to convince one person when several other people in line are sure they want the vaccine. But this illustrates the beauty of the church, that one person will always be worth it, and a fantastic reminder to me of God’s grace and relentless love for us.
God’s Call to his Church
In the end, we ended up hosting six clinics on the Eastside: three first-dose clinics and three second-dose clinics. Four of these clinics were hosted at our church in Lincoln Heights, while two clinics happened at our sister church in East Los Angeles. At our first clinic in Lincoln Heights, almost half of our patients came from our church’s immediate zip code (90031). At these six clinics, we were able to give out over 1750 doses to over 950 people. These clinics became the pilot that allowed other churches to distribute vaccines all across LA county. We know that every one of these people was a community member we had the privilege of serving. We now know many of these people: we were happy to see several people who came to our clinics start showing up to our church on the following Sundays. Others have stayed in contact with us in more minor ways; by watching our online service or following our social media. But we know that there were even more people served by these clinics who we only got to know briefly, but we know the clinic impacted in ways we will never see firsthand.
Often I see the Christian church in America respond to problems in our society in one of two unhelpful ways. The first posture is to dismiss social problems as not the church’s primary concern, instead of arguing that we need to focus on the church’s narrow role to preach and teach about Jesus. Under this view, getting caught up in the issues we see swirling around us is merely a distraction from the root problem, which is spiritual. The problem with this view is that it vastly simplifies the message of Jesus, ignoring the clear biblical mandate to be prophetic in the face of evil. Jesus started his ministry quoting Isaiah 61, saying he had arrived to “Proclaim good news to the poor” and “freedom for the prisoners.” The Bible is clear: our call is to speak into the social problems we see in our world because God himself is constantly speaking into social problems, from Genesis to Revelation, and most clearly in the person of Jesus. Over time, this perspective leads to a kind of cold, indifferent church that will fall away from its calling and is unlikely to convince the broader world its gospel has something to offer
The other posture is to broadly say that our job is activism, using the church primarily as a platform to speak truth to power prophetically when we see injustice. According to this view, social problems are fixable with enough activism; therefore, we must constantly use our political power to beat the drum for change. The problem with this view is that it often plays into a cultural trend towards a very abstract and hobbyist activism that ignores the difficulty of social change on two levels. First, it overestimates the ability of local churches to have a significant enough voice to influence a national or global political order where individual voices usually get ignored, and gridlock often reigns. Second, it often vastly simplifies how complex public policy-making is. It is easy to visualize public policy as pulling a switch to end injustice if only the powerful would care enough. Realistically, public policy is more like trying to troubleshoot an old electronic device, tinkering with controls, unsure whether a particular action will help us make progress or set us two steps back. Over time, this perspective leads either to burnout, disappointment at how little one could accomplish, or delusion, thinking that your discursive approach is creating change when you are often simply shouting into the void of Twitter.
I appreciated the opportunity to work on these clinics because it became a very concrete example of the possibility of a kind of “middle path” between these two tendencies. On the one hand, the clinics allowed us to address a real social problem (access to the vaccines). On the other hand, they allowed our church’s pastorally gifted leaders to pray and seek spiritual healing for people who needed and wanted spiritual guidance after a year of traumatic experiences. And we did so not by focusing on abstract activism but on leveraging our church’s resources to spur clear and concrete change for our neighbors on a local level where we knew we could see change happen. And I think this is a simple approach that will serve the vast majority of churches far better in the long run.